Incident Investigation Case Studies: Lessons from Real-World Failures

When something goes wrong in the workplace, the consequences can range from costly downtime to serious injury. Learning from real-world incidents is one of the most effective ways to prevent history from repeating itself. By studying what happened and why it happened through structured incident investigations, organisations can strengthen their safety culture and decision-making processes.
In this article, we’ll walk through three incident investigation case studies where digital tools and the 5 Whys method have been utilised to uncover the root causes and identify opportunities for improvement.
Case Study 1: Equipment Failure at a Car Manufacturing Plant
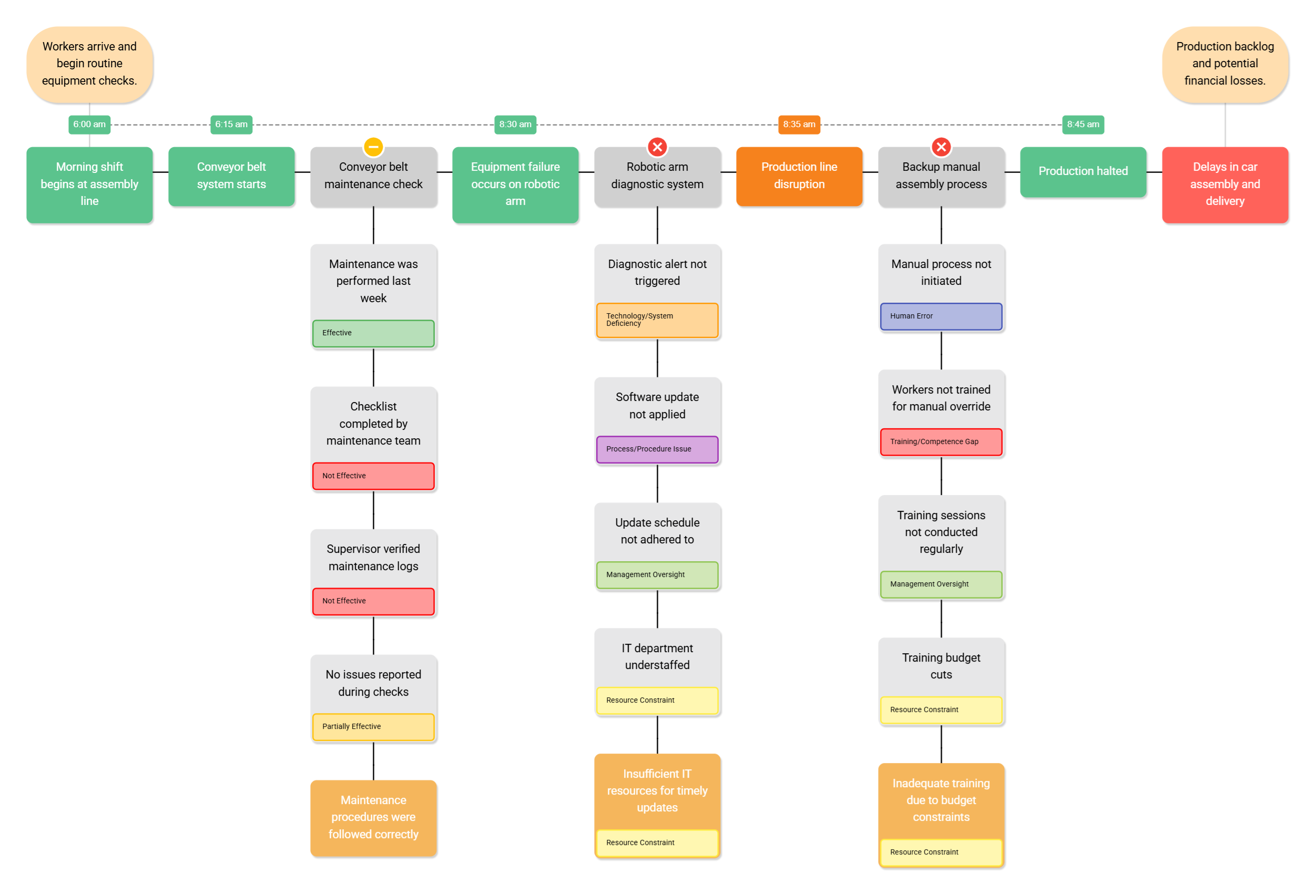
In a car assembly plant, a critical piece of machinery unexpectedly broke down at 8:30 am, immediately halting production and delaying car delivery.
Walkthrough of the Incident Investigation – Figure 1. Incident diagram of Equipment Failure at a Car Manufacturing Plant
5 Whys in Action
Investigators wanted to understand why this failure occurred, so they applied the 5 Whys investigation method (The 5 Whys Explained) to uncover the root cause. By repeatedly asking “why”, the team uncovered that the root cause was as follows: Insufficient IT resources for timely updates. Although the root cause has been identified, the investigation has flagged that there are far more potential system failures on the line. To understand the run up to this incident, the team started to breakdown and analyse the barriers in further detail using the 5 Whys method.
Barrier 1: Conveyor Belt Maintenance Check
Why was the conveyor belt maintenance check only partially effective?
-
Because maintenance was performed recently but did not detect any issues.
Why were no issues detected? -
Because the maintenance checklist was completed as per standard procedure without identifying abnormalities.
Why did the checklist fail to identify abnormalities? -
Because the inspection relied solely on visual checks rather than diagnostic testing.
Why were diagnostic tests not included in the procedure? -
Because the maintenance procedure had not been updated to include new testing methods.
Root Cause: Outdated maintenance procedure lacking detailed diagnostic checks.
Barrier 2: Robotic Arm Diagnostic System
Why was the robotic arm diagnostic system ineffective?
-
Because the diagnostic alert was not triggered.
Why was the alert not triggered? -
Because the latest software update was not installed.
Why wasn’t the update installed? -
Because the update schedule was delayed.
Why was the update schedule delayed? -
Because the IT department did not have enough staff to complete updates on time.
Root Cause: Insufficient IT resources to maintain timely software updates.
Barrier 3: Backup Manual Assembly Process
Why was the backup manual assembly process ineffective?
-
Because the manual process was not activated when automation failed.
Why wasn’t it activated? -
Because operators were not confident performing the manual override.
Why weren’t they confident? -
Because they had not received recent hands-on training.
Why hadn’t training been conducted recently? -
Because the training program was reduced due to budget constraints.
Root Cause: Inadequate operator training resulting from budget cuts.
To prevent future incidents of this nature, the car assembly plant should ensure sufficient IT resources, such as software updates and IT staff, to keep equipment up to date. They should also conduct regular training sessions to maintain operator competence and readiness for manual fallback processes.
Case Study 2: Trip & Fall in a Warehouse
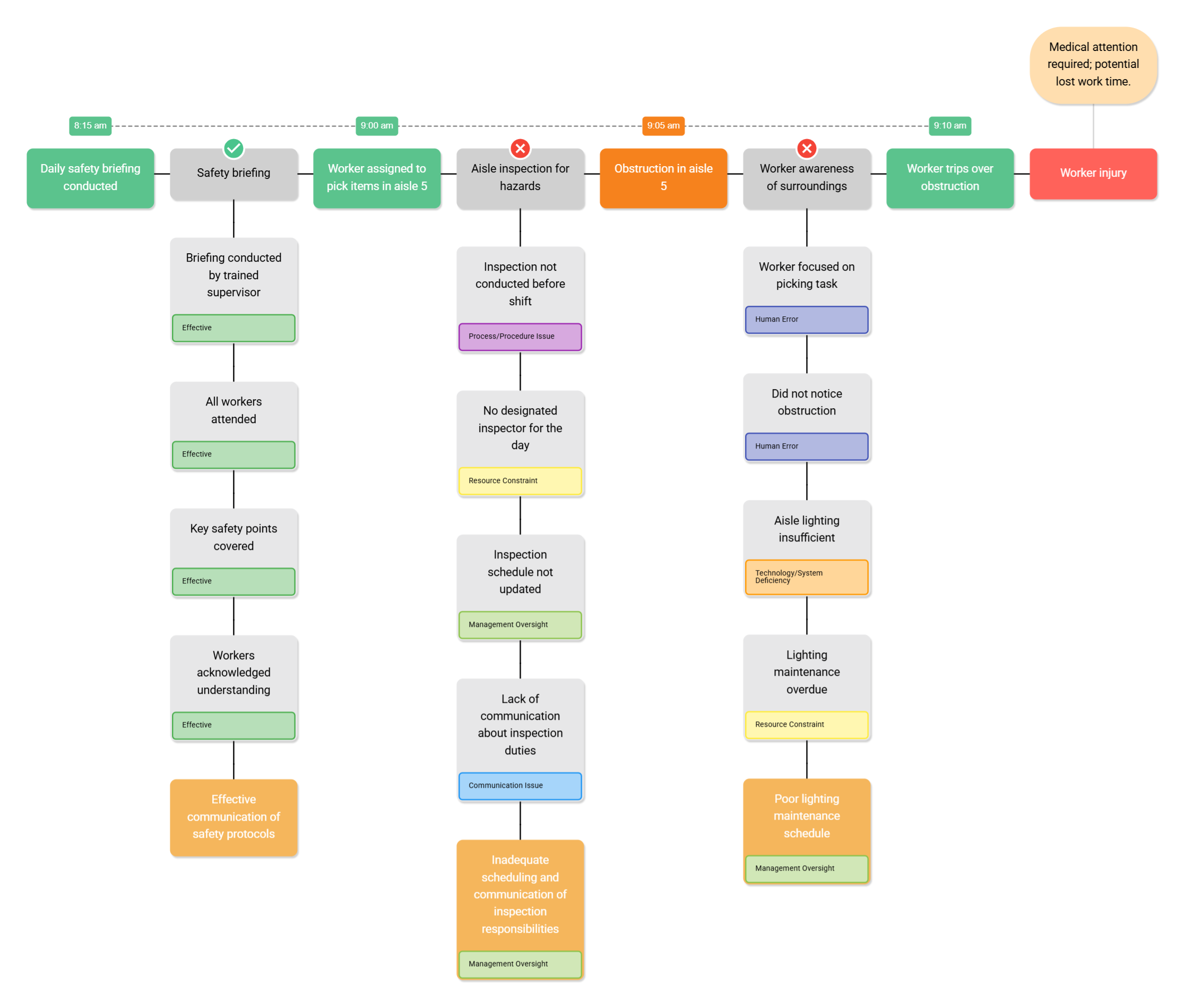
A worker tripped over an obstruction in a warehouse aisle at 9:10 am, resulting in a minor injury but raising concerns about workplace practices and communication.
Walkthrough of the Incident Investigation – Figure 2. Trip & Fall in a Warehouse
Investigators built a timeline of events, from the morning safety briefing to the moment of the trip, to understand the sequence and context of contributing factors.
5 Whys in Action
The team applied the 5 Whys method to analyse key barriers and identify the root cause.
Barrier 1: Safety Briefing
Why was the safety briefing effective?
-
Because it was led by a trained supervisor who followed the briefing procedure.
Why did the supervisor follow the procedure effectively? -
Because all workers attended and engaged in the briefing.
Why were all workers engaged? -
Because the key safety points were clearly communicated and discussed.
Why were the key points communicated effectively? -
Because the supervisor used visual aids and ensured workers understood before starting the shift.
Root Cause: Consistent and effective communication of safety protocols by trained supervisors.
Barrier 2: Aisle Inspection for Hazards
Why was the aisle inspection for hazards ineffective?
-
Because the inspection was not completed before the shift started.
Why wasn’t it completed? -
Because no one had been assigned to carry out the inspection that day.
Why wasn’t anyone assigned? -
Because the inspection schedule had not been updated for the new shift rotation.
Why hadn’t the schedule been updated? -
Because communication between supervisors about inspection duties was unclear.
Root Cause: Inadequate scheduling process and poor communication of inspection responsibilities.
Barrier 3: Worker Awareness of Surroundings
Why was the worker’s awareness of surroundings ineffective?
-
Because the worker was focused on completing a picking task.
Why was the worker so focused on the task? -
Because they were under pressure to meet a time target.
Why did the worker fail to notice the obstruction? -
Because the aisle lighting was too dim to clearly see hazards.
Why was the lighting dim? -
Because lighting maintenance had been delayed and not prioritised.
Root Cause: Poor maintenance scheduling and oversight of lighting systems.
The investigation revealed that this incident was not simply due to human error. Instead, it resulted from a combination of system weaknesses, including unclear inspection responsibilities, poor environmental conditions, and maintenance oversights. By strengthening communication channels, enforcing regular inspection routines, and improving environmental maintenance, the organisation can significantly reduce the risk of similar incidents in the future.
Case Study 3: Near Miss in a Gas Facility
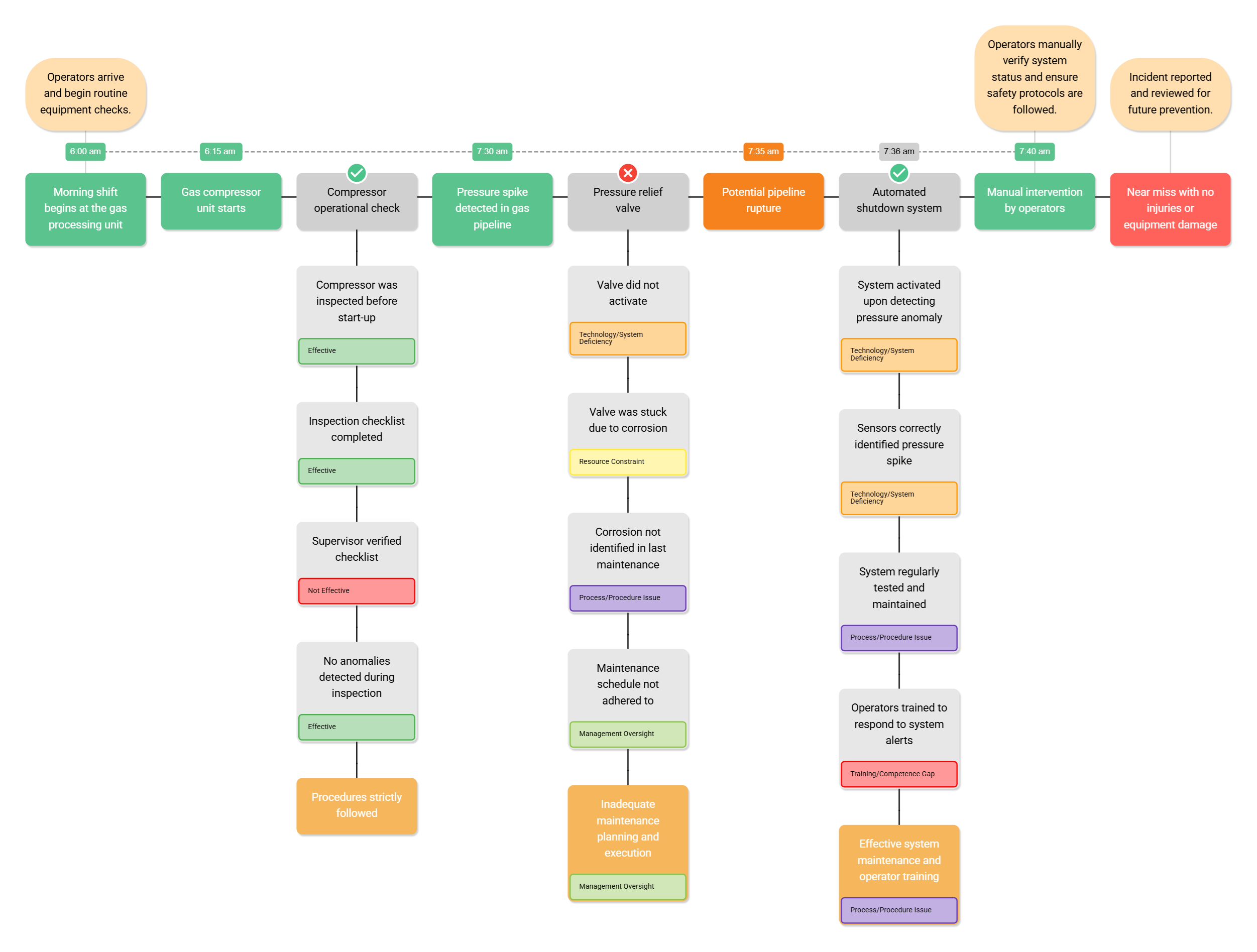
During a routine operation at a gas facility, a near miss occurred when a valve did not activate. Fortunately, no release occurred, but the severity of the incident warranted an investigation.
Walkthrough of the Investigation – Figure 3. Near Miss in a Gas Facility
In the timeline of events, 2 out of 3 barriers were functional (compressor operational check and automated shutdown system), while one was ineffective (pressure relief valve) Let us analyse these barriers.
5 Whys in Action
In the timeline of events, two out of three safety barriers were functional, the compressor operational check and the automated shutdown system while the pressure relief valve was found to be ineffective. Investigators applied the Five Whys method to understand why each barrier performed as it did.
Barrier 1: Compressor Operational Check
Why was the compressor operational check effective?
-
Because the compressor was inspected before start-up.
Why was it inspected before start-up? -
Because the inspection checklist was completed as part of the standard pre-start procedure.
Why was the checklist completed accurately? -
Because the supervisor verified each inspection step before authorising start-up.
Why did the supervisor’s verification process work well? -
Because no abnormalities were identified during the inspection and procedures were followed as designed.
Root Cause: Strong adherence to established inspection procedures and supervisory verification.
Barrier 2: Pressure Relief Valve
Why was the pressure relief valve ineffective?
-
Because the valve did not activate when pressure rose above safe limits.
Why didn’t the valve activate? -
Because it was seized due to internal corrosion.
Why was the corrosion not detected earlier? -
Because it was missed during the last scheduled maintenance check.
Why was it missed during maintenance? -
Because the maintenance schedule was not consistently followed or reviewed.
Root Cause: Inadequate maintenance planning and inconsistent execution of inspection routines.
Barrier 3: Automated Shutdown System
Why was the automated shutdown system effective?
-
Because it successfully activated when a pressure anomaly was detected.
Why did it activate correctly? -
Because the system’s sensors accurately identified the pressure spike.
Why were the sensors functioning correctly? -
Because they are regularly tested and maintained as part of routine checks.
Why are these maintenance routines effective? -
Because operators are well-trained to manage and respond to system alerts.
Root Cause: Effective preventive maintenance program supported by well-trained operators.
The investigation confirmed that this near miss was prevented by the reliability of two key barriers; the compressor check and the automated shutdown system. However, the pressure relief valve failure exposed weaknesses in maintenance planning and execution. To prevent future near misses, the gas facility should consider reinforcing maintenance planning and scheduling to ensure all critical safety devices are thoroughly inspected. Alongside this the facility should continue investing in operator training and regular system maintenance to preserve the effectiveness of automated safety systems.
Overall Conclusions
Incidents, whether failures, accidents, or near misses, hold invaluable lessons. By using digital incident investigation software, organisations can transform setbacks into opportunities for learning and prevention. With the right approach, failures don’t just highlight what went wrong, they guide us toward building safer, more resilient workplaces. Incident Insight makes this process simpler and more effective. From mapping timelines to analysing root causes and tracking corrective actions, it helps teams uncover what really happened and ensure it doesn’t happen again.
Ready to see how Incident Insight can support your organisation’s investigations? Send us a message at support@salus-suite.com.